
Temporomandibular joint
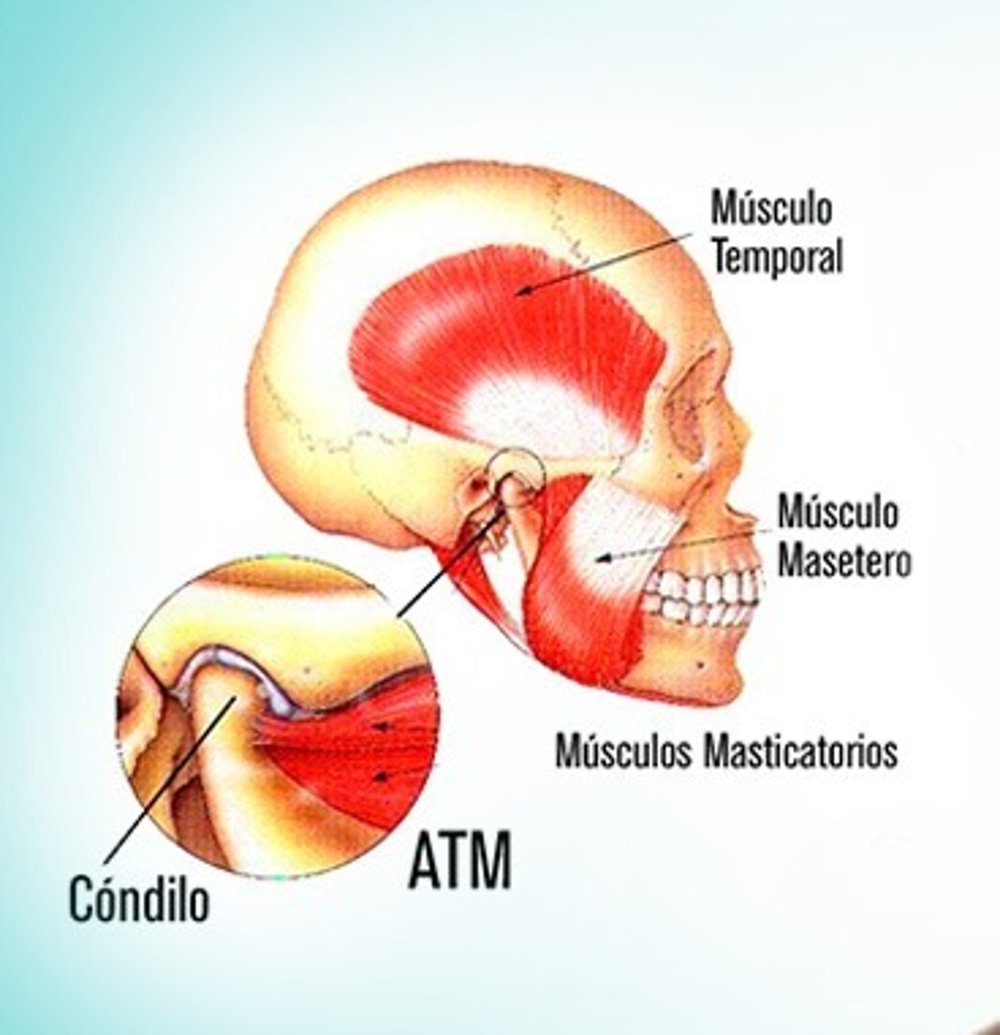
The TMJ is the joint between the temporal bone and the jaw (temporomandibular joint) and is located in front of the ears and is used when we speak, chew or swallow. It is the joint responsible for mouth movements. We therefore have two TMJs, one on each side of the face connecting the jaw (in a horseshoe shape) to our head. Between this joint there is a fibrocartilaginous articular disc that facilitates jaw movements, in turn it is inserted into ligaments that stabilize this disc in the correct position. Surrounding this joint there is also a joint capsule composed of muscles, blood vessels and nerves. Of all the joints in the body, the TMJs are the ones that concentrate the largest number of nerve endings, which is why they are commonly affected by painful disorders.
TMJ Dysfunction
TMJ dysfunction is the abnormal functioning of the temporomandibular joint, ligaments, chewing muscles, maxillary and mandibular bones, teeth and dental support structures. Just as wearing inadequate footwear for a long time causes injuries to the joints of the feet and knees, unbalanced chewing, tooth loss, postural problems, undesirable nighttime habits, or even habits such as biting nails, cuticles or even chewing gum excessively, cause injuries to the TMJ. At first, small noises (clicking) are noticed when opening and closing the mouth. Over time, these noises may be accompanied by pain, deviations in the mouth opening trajectory, difficulty chewing and pain when chewing, limited mouth opening, headaches, earaches and even tinnitus. Temporomandibular dysfunction (TMD) can occur in both children and adults. The incidence is equal in men and women. Painful symptoms are more frequent in women.

Treatment of TMJ Dysfunction
The treatment of temporomandibular disorders always depends on the correct diagnosis of the pathology. Diagnosis of these disorders is complex due to the multifactorial nature of the disease and is not always obvious. The history of the disease's progression, a detailed anamnesis, clinical and physical examinations and imaging tests such as x-rays, CT scans and MRI are essential for the correct diagnosis. Once the diagnosis is confirmed, we can develop a treatment plan that can be conservative or surgical.
Clinical Treatment
Conservative treatment consists of rehabilitating the occlusion and stabilizing the patient's stomatognathic system, and many therapeutic resources can be used, such as: dental implants to replace lost teeth, use of orthodontic appliances to level and align the dental arches, bite plates to protect the teeth from clenching and promote muscle relaxation and relief from painful symptoms, physiotherapy with local heat, electrostimulation, use of therapeutic laser, acupuncture, anti-inflammatory and muscle relaxant medications, hypnosis, use of botulinum toxin and viscosupplementation.
The choice of conservative treatment method will depend on the diagnosis, the chronicity of the lesion and the intensity of the signs and symptoms.
Occlusal splint
Laser
Botulinum toxin
Viscosupplementation
Tratamento Cirúrgico
Surgical treatment of dysfunctions is indicated when we detect physical disorders of the joint structures, which may have immediate indications for surgery or when conservative treatment has failed to restore joint harmony and the signs and symptoms return or even increase over time. We should never think that surgical treatment is the last resort for treatment, as this will certainly lead to treatment failure, since there are specific indications for surgical treatment, that is, when there is impairment of function, caused by changes in morphology, followed or not by complaints of pain. Surgical treatment acts directly on the joint, correcting any internal disorders of the joint, promoting a change in the altered or diseased anatomical structure, restoring masticatory function and relieving painful symptoms.
Articular disc displacement is considered the most common articular pathology of the TMJ and is characterized by a malpositioned relationship of the articular disc in relation to the head of the mandible (condyle).
This articular disc displacement can be classified as: displacement with reduction and displacement without reduction.
In displacement with reduction, during mouth opening, the disc is repositioned, at which point a joint popping sound can be heard, the mouth opening remains within a limit considered normal and when the mouth is closed, the disc is again displaced to its previous position and a new popping sound can be detected, with or without painful symptoms. Displacement without reduction is the evolution of an untreated or improperly treated displacement with reduction. In this type of displacement, limitation of mouth opening is often associated because during mouth opening the head of the mandible pushes the articular disc even further anteriorly, causing compression of the retrodiscal tissues and generally severe pain. Chronicity of disc displacement without reduction promotes deformations of the disc, perforations, adhesions and consequently restriction of mouth opening and increased painful symptoms.
Types of TMJ Surgery
There are specific methods with precise indications for each technique. However, in general terms, we can consider the surgical approach to TMJ as closed or open surgery.
Closed surgery is performed using state-of-the-art equipment, called arthroscopes. With the advent of TMJ arthroscopes, it is possible to perform TMJ surgery without incisions, just 2 or 3 small holes through which the instruments and fiber optics enter.
Open surgery is when there is a need to cut the skin and perform a surgical access that allows direct visualization. In open TMJ surgery, the incision is made near the ear fold and the scar is not usually a cause for concern.
Joint Replacements
Joint replacements or joint reconstructions are performed when we have an advanced case of joint degeneration due to osteoarthritis/arthrosis, when the joint is affected by a large cyst or tumor, or even when it is affected by an explosive fracture of the mandibular head. Joint reconstructions can be performed with bone grafts or joint prostheses.
Joint prostheses can be divided into 2 groups:
1- Standard or "off-the-shelf" prostheses, which are prefabricated and stored on the shelf for immediate emergency use.
2- Customized or personalized prostheses, which are individualized for each individual, through computed tomography associated with the CAD-CAM process. These are superior in terms of adaptation, shorter surgical time and therefore make the surgery safer.